By Divya Pandey and Anna Bolgrien
In a research project combining data from IPUMS MICS and IPUMS DHS, IPUMS Global Health staff examined trends in the relationship between open defecation and high infant mortality rates (IMR) in the Eastern Indo-Gangetic Plains. The project focused on selected bordering regions in Nepal, Bangladesh, and India. By analyzing these environmentally and agro-climatically comparable regions, the study aimed to isolate the impact of national and local policies on open defecation and infant mortality rates.
Figure 1: Regions included in the study

The study pooled data from IPUMS MICS and IPUMS DHS to look at trends over almost two decades. IPUMS DHS includes data for all three countries, and IPUMS MICS provides additional years of data for Nepal and Bangladesh. Since the study focused on selected bordering geographies, the authors worked with data from lower administrative levels—divisions in Bangladesh, states in India, and regions in Nepal. Leveraging the geography resources provided by IPUMS, the team used both spatially harmonized and sample-specific geography variables (learn more about IPUMS DHS geography variables and IPUMS MICS geography variables). Spatially harmonized geography variables identify geographic regions using a consistent spatial footprint to allow for the comparison of the same physical space over time. Sample-specific geography variables are not harmonized across time; as their name suggests, they use the geographic boundaries that are sample-specific or contemporaneous to the survey-year in a country.
Identifying comparable subnational geographies
For India, the authors relied solely on IPUMS DHS data. They used the spatially harmonized geography variable for India to isolate data for the states of interest (Bihar, West Bengal, Uttar Pradesh).
For Bangladesh, the spatially harmonized variables from IPUMS DHS (see IPUMS DHS variable GEO_BD1994_2018) and IPUMS MICS (see IPUMS MICS variable GEO1_BD) are comparable for the divisions of Rangpur and Rajshahi. The Nepal subnational geography posed greater challenges; different geographic classifications over time limit the comparability between IPUMS DHS and IPUMS MICS geographic units. The study focused on the Terai region. IPUMS DHS initially defined regions by broad development zones (2001, 2006), then by ecological zones (2011), and later by provinces (2016). IPUMS MICS, on the other hand, included data for development zones in the earlier rounds (2010, 2014) before transitioning to provinces in 2019. The resulting difference can be seen in Figure 2 below, where (a) represents the spatially harmonized IPUMS DHS geography and (b) represents the sample-specific IPUMS MICS 2019 geography, which reflects Nepal’s provinces.
Figure 2: Lower administrative level boundaries for Nepal in IPUMS Global Health Projects
Given the inconsistencies between the two geographies and the longer time horizon of the DHS data and spatially harmonized geographic variable, the study uses only IPUMS DHS data for Nepal.
Results
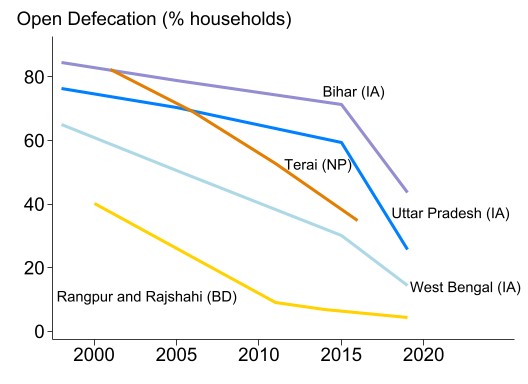
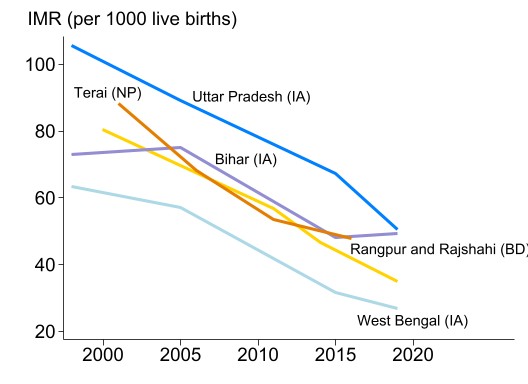
Analysis revealed that open-defecation and IMR have both been declining in the Eastern Indo-Gangetic Plain, as shown in Figure 3. Nonetheless, open defecation continues to be a significant determinant of infant mortality. After controlling for the women’s religion, age, education, urban/rural status, the child’s sex, and the time trend, a household’s practice of open defecation is associated with a 0.8 percentage point increase in the probability of death during a child’s first year of life. These associations are strongest for the subregions in India and Nepal. In contrast, the authors do not find a significant relationship between open defecation and IMR in Bangladesh, highlighting the public health gains from widespread access and use of improved sanitation facilities and reduced open defecation in the country. This divergent outcome suggests that Bangladesh offers lessons for India and Nepal in advancing public health through sanitation improvements.
Figure 3: Open Defecation and Infant Mortality Rate (IMR)