
By Miriam L. King and Sula Sarkar
IPUMS DHS now includes integrated variables for 84 counties (up from 51) and nearly 350 samples (up from 233), including new data from Latin America, Eastern Europe, Oceania, the Caribbean, and Central and East Asia. Providing DHS data in a form that facilitates micro-analyses across countries is one of IPUMS’ greatest strengths, so researchers will be excited to learn that they can now do even more! Our latest data release expands the scope of IPUMS DHS beyond its initial coverage of Africa, the Middle East, and South Asia and adds the latest samples for 12 countries previously in the database. Figure 1 shows the full geographic scope of IPUMS DHS, as well as highlighting newly added countries and previously included countries with new samples.
Figure 1: Countries included in IPUMS DHS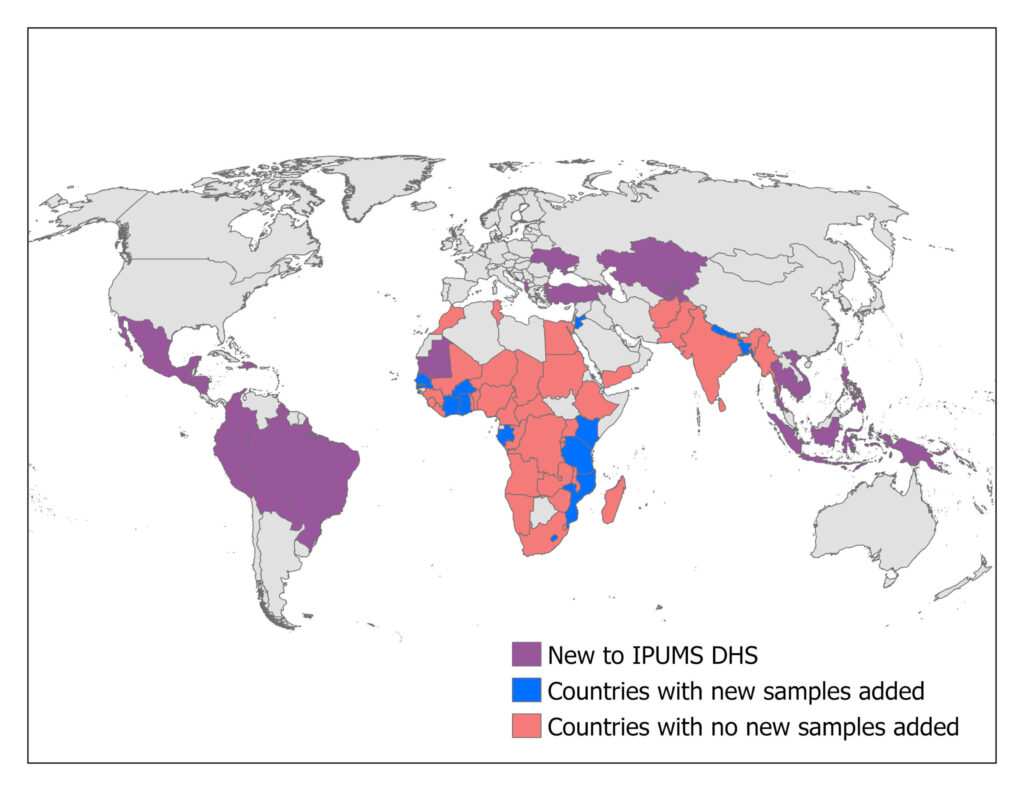
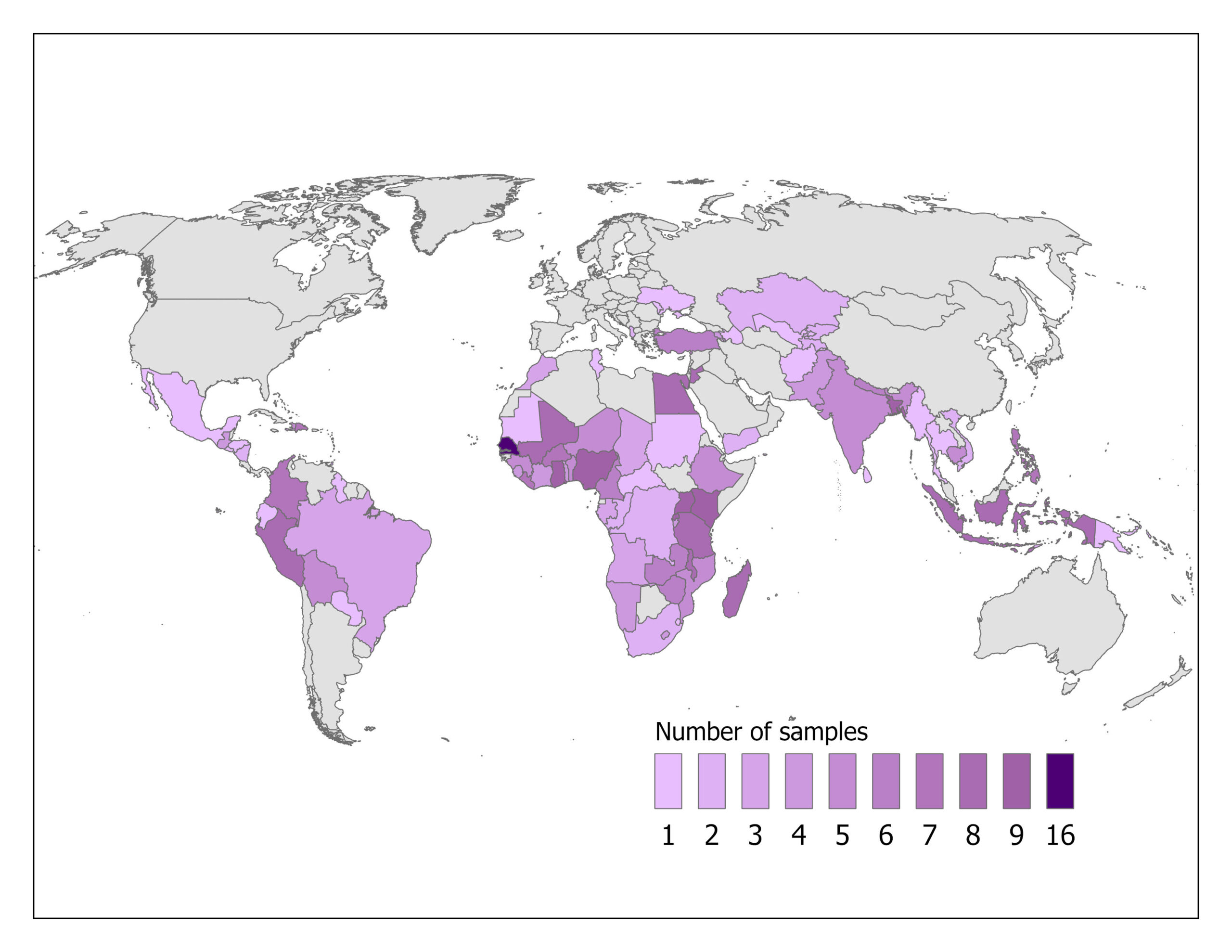
IPUMS DHS facilitates comparative analysis across time as well as across space. Figure 2’s map of included countries summarizes the potential for cross-temporal analysis, by using increasingly dark coloring to document growing numbers of samples. Three-quarters of the countries included in IPUMS DHS have more than one sample, allowing for analysis of change over time.
Figure 2: Number of samples in IPUMS DHS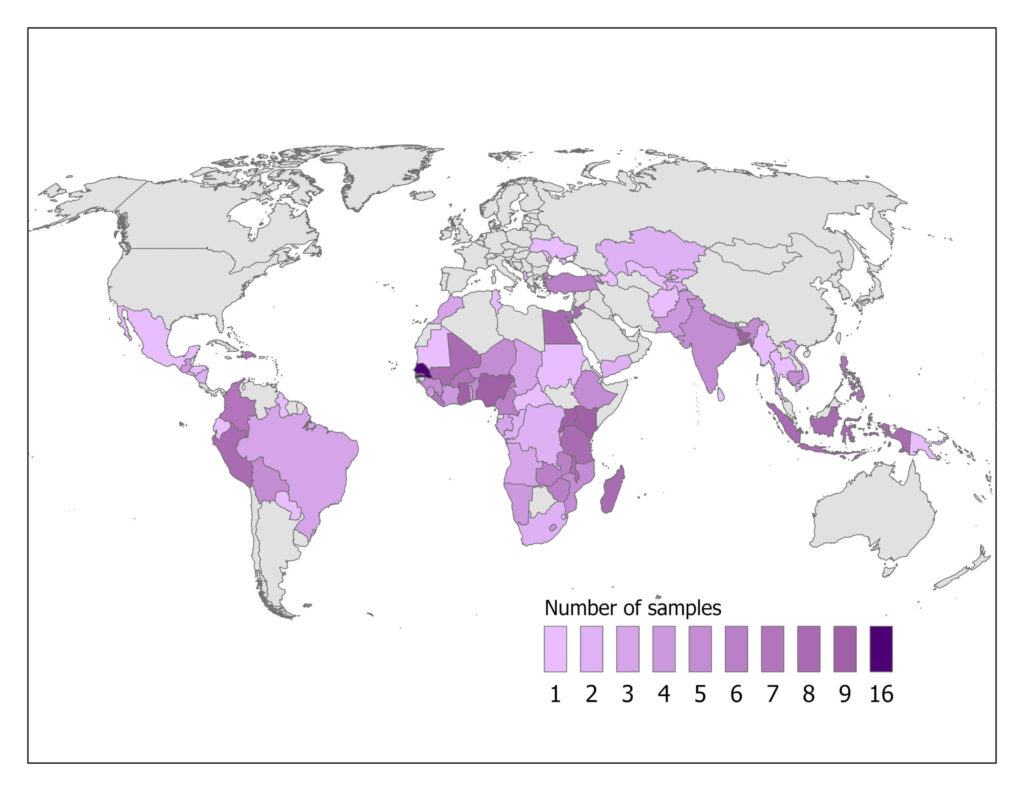
The recent IPUMS DHS data release includes 13 samples from DHS Phase 8 and adds over 200 new variables from that Phase. These variables introduce new topics, including HPV vaccination, symptoms and treatment of depression and anxiety, management of menstrual periods, self-reported health status, and early child development.
Adding material from 115 samples in the latest data release required IPUMS DHS staff to set priorities, rather than harmonizing every variable from every sample. First, we integrated variables for women, young children, births, and household members, but we delayed harmonizing data for men until another release planned for 2026. Second, we skipped country-specific variables and focused on widely available standard variables. Among the variables with standard names, we skipped those based on open-ended questions about “where” something took place (e.g., where you could get contraception) or “who” did something (e.g., who assisted with delivery), because their responses varied widely across samples. Finally, we held off on releasing data from pregnancy histories and on pregnancies as a new unit of analysis; that material will be a priority for our next project phase.
The new data in IPUMS DHS opens the door to exciting opportunities for truly global health research. While analysts of health and well-being in Africa and South Asia have used IPUMS DHS for over a decade, scholars focusing on other world regions or on the globe as a whole now have a rich new resource for their research.