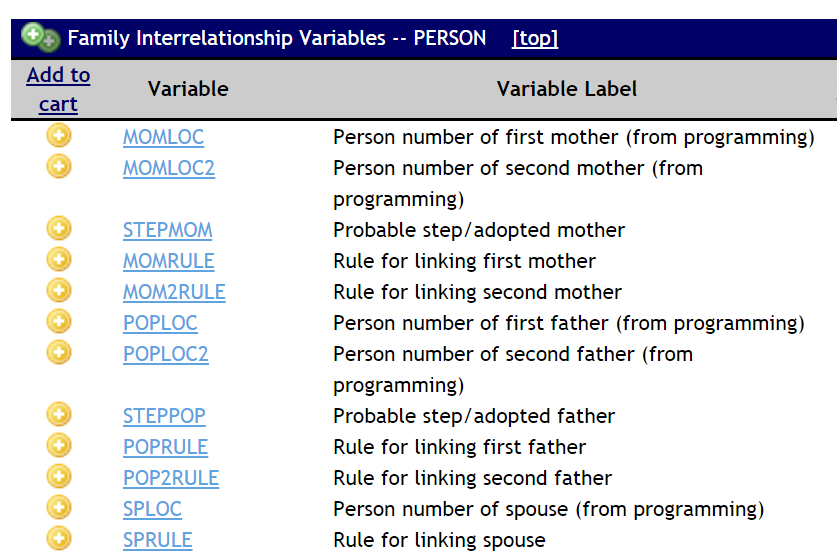
IPUMS has updated the family interrelationship variables in IPUMS CPS and the Integrated Health Interview Series (IHIS) to include same-sex and cohabiting couples. The updated variables dramatically reduce research barriers for those interested in this family and household context.